

Abstract
Background: Successful engraftment remains a challenge in hematopoietic cell transplantation (HCT) for some patients. Salvage approaches, including use of recombinant hematopoietic growth factors, cytokine therapy, CD34+-selected progenitor cell boosts, or second or subsequent HCT, are successful only in a minority of patients, and patients are exposed to prolonged blood products transfusions. With our successful pre-clinical rodent and Rhesus Macaques total body irradiation injury-induced marrow failure models (Metheny, Front Med 2018; Sher, Cell Transplantation 2018; Sher, Blood 2017), this prospective, multi-center, phase I clinical trial is evaluating the safety of PLX-R18 cells used to improve peripheral blood counts in patients who have experienced incomplete hematopoietic recovery after HCT. PLX-R18 cells are human placental-derived adherent stromal cells that are predominantly of fetal origin, expressing CD105, CD73 and CD29, and lacking surface expression of CD45, CD34, CD14, CD19, HLA-DR, CD31 (endothelial marker) and GlyA (erythrocyte cell marker). PLX-R18 also do not express HLA class II molecules (HLA-DP, DQ, and DR) and co-stimulatory markers (CD80, CD86, and CD40). PLX-R18 cells secrete MCP-1, IL-6, and IL-8 and had been shown to stimulate migration of bone marrow cells in vitro. Cells are grown ex vivo, under GMP conditions, using a 3-dimensional system, and are administered as several intramuscular (IM) injections. PLX-R18 cells already are approved for treatment of acute radiation syndrome (ARS) under an IND.
Methods: This is a multi-center, open label, dose-escalation, phase 1 trial (ClinicalTrials.gov: NCT03002519). Eligibility criteria include patients age ≥18 years who underwent either an autologous (auto) or an allogeneic (allo) HCT but had incomplete hematopoietic recovery at 4 months post-transplant, defined as failure to maintain either hemoglobin (Hb) >8 g/dL and/ or neutrophil count (ANC) >1,000/µL and/or platelet count (Plt) (unsupported) >50,000/µL. Other eligibility criteria include ECOG performance status of 0-2, no evidence of underlying malignancy at time of enrollment, no active infection, and no evidence of grade 3-4 acute or severe chronic GvHD. The PLX-R18 cells, cryopreserved in DMSO and human serum albumin in Plasma-Lyte, are thawed and injected IM in multiple locations - half into the gluteus medius muscle on one side and half to the thigh muscles on the contralateral side. A total of 24 subjects are planned to be enrolled into 3 dose escalating cohorts: low (n=3) given 1 million cells/kg; intermediate (n=6) at 2 million cells/kg and high (n=15) dosed at 4 million cells/kg each. The assigned dose is given twice, 1 week apart; cohorts are recruited sequentially and progression to the next cohort is based on the safety assessment of its predecessor. Adverse event is graded using the CTCAE criteria of the NCI. As of July 2018, all 3 patients of cohort 1 were treated (with sufficient follow-up), as well as 3 out of the 6 subjects planned for the 2nd cohort, and data of the first cohort are presented herein.
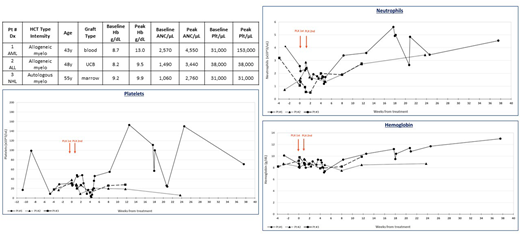
Results: Cohort 1 (low-dose) - 3 subjects (ages 43, 48 and 55 years old) who had an allo (n=2) or auto (n=1) HCT received two IM administrations of PLX-R18, 1 million cells/kg each within a 1-week interval. 67 Adverse Events (AEs) were recorded. 64.3% of the AEs were grade 1, 30.9% were grade 2, 3.6% were grade 3 and 1.2% were grade 4. One patient suffered from 3 Serious AEs (immune thrombocytopenic purpura, bacteremia and migraine), all assessed as not related to treatment. Most frequent related AE was transient injection site pain, experienced by all 3 patients. See patients' details and blood counts in the table and graphs.
Conclusions: Treatment with PLX-R18 generally was well-tolerated and most frequent adverse events were injection site reactions, which were all reversible without sequelae. The trial continues to accrue patients and the next dosing cohort (intermediate dose) is at 2 million cells/kg.
Upon completion, a larger phase II trial will be considered in the same indication using the optimal dose. Other potential uses include PLX-R18 therapy in Acute Radiation Syndrome, Bone marrow failure, and in HCT as a "pan" cytokine for rapid count recovery.
Lazarus:Pluristem Ltd.: Consultancy. Zuckerman:Cellect Biotherapeutics Ltd: Consultancy. McGuirk:Novartis Pharmaceuticals Corporation: Honoraria, Other: speaker, Research Funding; Fresenius Biotech: Research Funding; Kite Pharma: Honoraria, Other: travel accommodations, expenses, speaker ; Gamida Cell: Research Funding; Astellas Pharma: Research Funding; Pluristem Ltd: Research Funding; Bellicum Pharmaceuticals: Research Funding. Rosen:Pluristem: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal